Documentation
·
5 min read
Discover 4 effective strategies to optimize your physical therapy documentation process and reduce the time spent on note-taking. Learn how to streamline your workflow and increase efficiency, so you can focus more on providing quality…
PS
The PatientStudio team
Practice operations

Do you ever feel like you spend more time on notes than on providing quality care to your patients? If you’re a physical therapist, documentation is a critical part of your job, and it’s essential for compliance and delivering evidence-based care that is tailored to each patient’s needs. Physical therapy documentation is the process of recording all relevant details of a patient’s treatment, from medical history to progress and treatment plans. In this post, we’ll explore what physical therapy documentation is, why it’s so important, and 4 effective ways to optimize your documentation process and save time without sacrificing quality of care. Click here to jump right to the 4 strategies.
What are the Challenges of Physical Therapy Documentation?
Physical therapy documentation is a necessary part of providing quality care to patients, but it can also be a major source of frustration and stress for physical therapists. Some of the main challenges include:
Time-consuming: Physical therapy documentation can be very time-consuming, taking up a significant portion of a physical therapist’s day. Oftentimes the time spent documenting notes is “unpaid” hours. This can make it difficult to balance the documentation requirements with other aspects of patient care and/or running a clinic.
Complex regulations: Physical therapy documentation is subject to complex regulations, such as HIPAA and Medicare guidelines, which can be difficult to navigate and adhere to.
Data management: Physical therapy documentation generates a large amount of patient data, which needs to be accurately recorded and securely managed. This data is cruicial to tacking patient outcomes and medical necessity. This can be challenging, especially for practices with limited resources.
Limited training: While most therapists are highly educated in anatomy, evaluation and treatment. Many physical therapists may not receive adequate training on how to document effectively or “defensibly”, which can result in errors and inconsistencies in documentation.
Technological barriers: Some physical therapists may face technological barriers to effective documentation, such as a slow or “clunky” electronic health record systems.
Addressing these challenges is crucial to ensure that physical therapy documentation is accurate, compliant, and effective in providing quality care to patients.
Why is it important to minimize physical therapy documentation time?
The lengthy documentation time can significantly impact a physical therapist’s ability to provide quality care to their patients. Physical therapists must record all relevant details about a patient’s treatment, including medical history, progress, evaluation, treatment plan, and goals. This documentation process can take up a significant portion of a therapist’s time and energy, leaving them with less time to focus on direct patient care. As a result, physical therapists may feel overworked and stressed, leading to burnout.
Moreover, the use of aging or legacy EHR software can also contribute to physical therapist burnout. While these software programs were origionally designed to improve the efficiency and accuracy of documentation, older software can be clunky and time-consuming to use. Many physical therapists report that navigating EHR software can be difficult and confusing, requiring them to spend more time on documentation than is necessary. In fact, according to a recent study, around 70% of therapists report that the speed of documentation using their EHR was the biggest factor contributing to burnout.
Strategies to Reduce Time Spent on Physical Therapy Documentation
1. Utilize Templates
Utilizing templates allows physical therapists to quickly and easily complete documentation without having to start from scratch. Templates can also be customized to provide more specific information, allowing physical therapists to provide more detailed documentation in less time.
Many clinics are likely to see the same types of patients repeatedly, depending on the patient demographic and referral sources. For example if a practice gets a steady amount of patients in recovery from ACL surgery, the therapists might consider starting from a “Postoperative Lower Extremity” template. This template could start with specifics such as a semi-written subjective narrative and prior level of function. Ideally, the objective section would have measures for pain scale, Lower Extremity Functional Scale (LEFT), Strength, ROM and potentially GAIT.
2. Automate Data Entry
Automating data entry allows physical therapists to quickly and easily enter patient data into their documentation system. This eliminates the need for manual data entry and saves time.
The best place to start is with Online Patient Forms. By creating a digital intake process you can automate the collection of patient demographics, medical history, medications, chief complaint and more. Additionally, by moving away from paper, clinics can completely eliminate printing, scanning, shredding and manual EHR data entry.
3. Utilize Pull Forward Documentation Software.
Physical therapy documentation software typically includes a feature called “copy forward” that allows therapists to easily populate fields in a new therapy note with information from a previous note. This can save time and ensure that important details are not missed or entered incorrectly. Copy/pull forward fields typically include things like the patient’s name, diagnoses, measures collected, and current treatment plan.
This can also include subjective information about the patient’s progress and any changes to functional abilities. By using copy forward fields, therapists can quickly and accurately document their interactions with patients and track their progress over time.
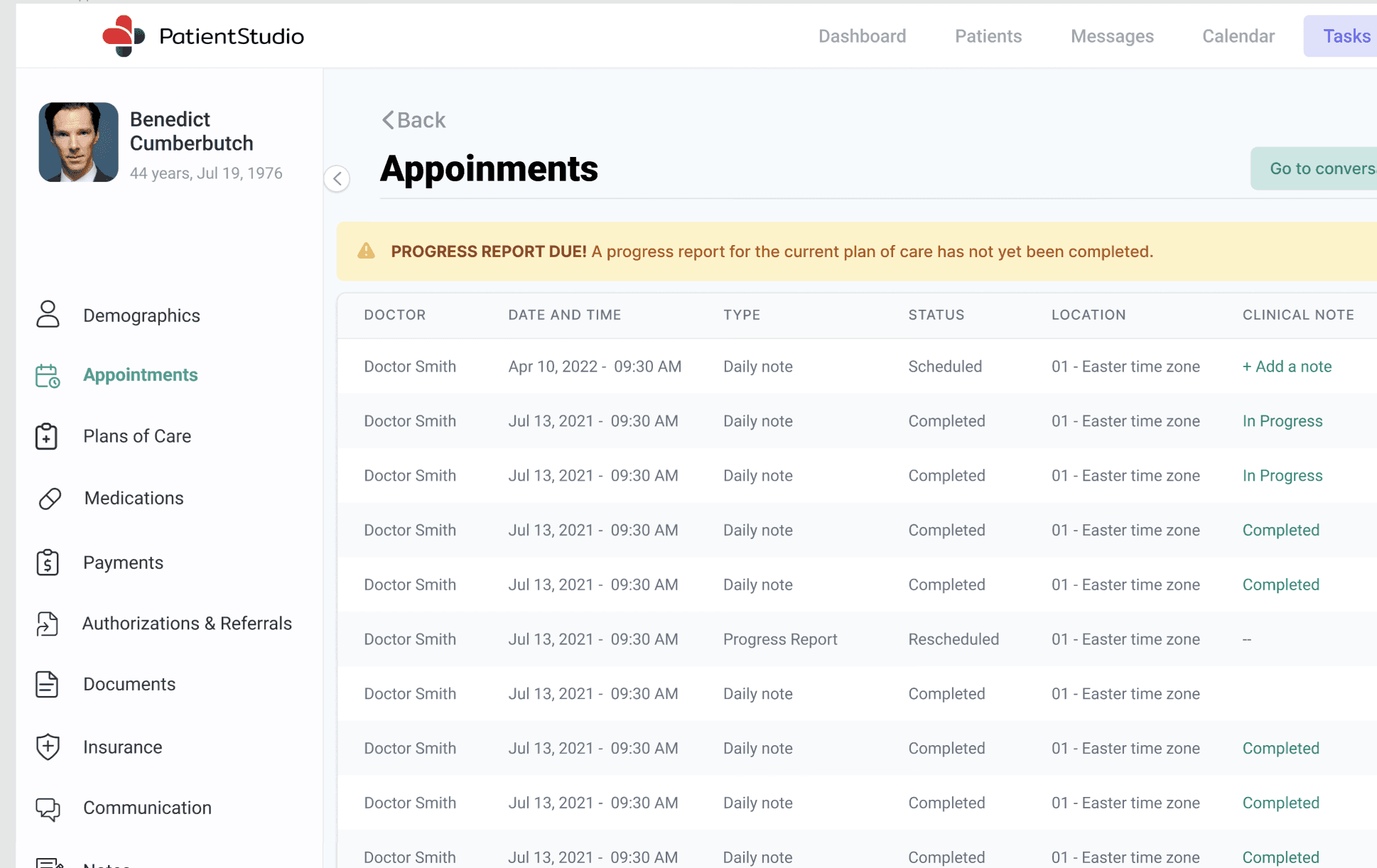
4. Utilize Progress Note Reminders
According to the Medicare Benefit Policy Manual, physical therapy progress reports must be submitted at least once every 10 treatment days. The first day of treatment, whether it is an evaluation, reevaluation, or actual therapy, marks the beginning of the first reporting period. The progress report period ends either on the 10th treatment day or on a date chosen by the therapist, whichever comes first. The next treatment day marks the beginning of the next reporting period.
Modern physical therapy documentation software should track the sessions remaining until a progress report is due. This would alert the therapist to complete a progress note by the 10th visit, in order to remain compliant with CMS standards.
Benefits of Reducing Time Spent on Physical Therapy Documentation
Reducing the time spent on physical therapy documentation can provide numerous benefits to both therapists and their patients. For therapists, it can free up more time to focus on providing direct patient care and can reduce the risk of burnout. For patients, it can lead to more efficient and effective treatment plans, as therapists will have more time to devote to developing and updating these plans.
Spending less time typing out notes has a direct correlation to employee morale and reducing staff burnout. Overall, reducing the time spent on physical therapy documentation can lead to better outcomes for both therapists and their patients.
Find out what your practice is leaving on the table
A 30-minute walkthrough of billing, verification, and the AI agents — on your numbers.